Breast

Breast Augmentation
Mr. Platt performed his first breast augmentation over twenty years ago and has extensive experience in the use of round and shaped (anatomical) implants used both in the subglandular and partial submuscular or dual plane technique. He is therefore able to tailor the surgery to the patient’s needs and tissue type. He uses a very bloodless technique to make the pocket and so drains are very rarely used in any of his breast surgery.
Mr Platt has extensive experience in the use of textured implants such as Mentor and Inamed as well as Polyurethane coated implants. He regularly deals with complex cases such as asymmetry, chest wall deformity or revision cases involving removal of capsular contracture or simultaneous mastopexy combined with augmentation.
Breast augmentation surgery takes place under general anaesthetic and involves an overnight stay. The scar is placed close to the crease under the breast and dissolving stitches are used. You may feel discomfort and hardness in the breasts following your operation, including some swelling and bruising. These symptoms can be managed with painkillers, but may last a few weeks. Scars should fade continuously for the next twelve months.
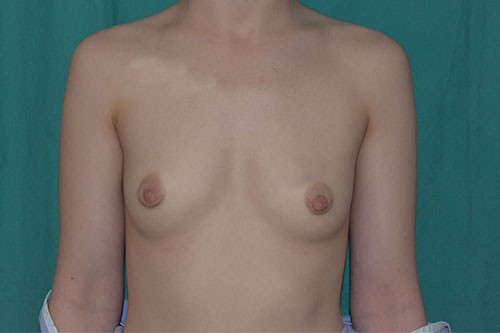
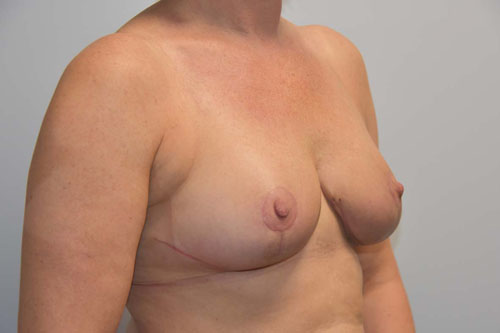
22 years old. Breast Augmentation with 335cc shaped implants placed in a submuscular dual plane position





Breast Augmentation with 245cc shaped implants placed in a submuscular dual plane position






Bilateral breast augmentation. 30 years old. 250cc shaped polyurethane implants placed in a dual plane submuscular pocket. 3 years post surgery.






Bilateral breast augmentation. 30 years old. 450 cc round polyurethane implants. 3 months post surgery.






Bilateral breast augmentation. 260 cc round polyurethane implants. 12 years post surgery.






Breast augmentation with 330 cc round implants placed in the subglandular position.






Breast augmentation. 45 year old patient with mild ptosis and asymmetry wanting enlargement with upper fullness but not wanting scars from uplift. Augmentation only in dual plane placement with 320cc round implants.






30 yrs old BBA with 620 cc round subglandular silicone implant. Photos takes 3 months post op.






Breast Reduction
Breast reduction can help relieve the physical symptoms associated with large or heavy breasts such as:
- Breast discomfort
- Neck ache
- Backache
- Shoulder pain
- Skin irritations underneath the breast fold
- Problems with clothes
- Indented bra-straps
- Difficulties and discomfort during exercise
55 year old troubled by very heavy uncomfortable breasts treated with breast reduction 2Kg on right and 2.3 Kg on left with free nipple grafts and a post op view at 6 weeks


Bilateral breast reduction. 40 years old. 460 gram reduction each side with an inferior pedicle technique and superior pedicle to suspend tissues. 2 months post op.





Bilateral Breast Reduction. 37 years old. Inferior pedicle technique, 470 gms removed each side, Pre and 1 month post op photos.






Bilateral breast reduction. 60 year old lady with physical symptoms of heavy breasts with discomfort. Body mass index 40 with type 2 diabetes. 1.15 Kg removed from Left and 0.94 Kg removed from Right using an inferior pedicle technique. 1 month post surgery photos.






How is the surgery performed?
Mr Platt uses an inferior pedicle technique for most of his breast reduction surgery. He has used this technique for over twenty years but modified and improved it along the way to suit individual patient’s needs. He adapts it according to the patient’s tissues and general health. Fit patients with good tissues and blood supply will be able to have more internal shaping of the tissues. The nipple is lifted into a new position and kept alive on a pedicle, or stalk, of tissue. Excess skin and breast tissue is then removed, and the remaining breast tissue reshaped to create a smaller and more elevated breast. An anchor-type incision or inverted T scar is used. Liposuction is used to flatten the sides of the chest wall when necessary.
At your first consultation you will be asked what is bothering you about your breasts and about your expected outcome from the surgery. You will be examined and some discussion will follow about scar patterns and what size of reduction is appropriate. If you are considered suitable you will be told about the operation, the expected outcome and possible risks and complications.
What should I expect in terms of treatment, procedures and outcomes?
Breast reduction surgery involves fairly complex operations that take between one-and-a-half to three hours to perform. The operation is carried out under general anaesthetic. You can expect to stay in hospital for one or two nights. You will have some dressings on your breasts or a thin layer of glue that acts as a dressing. You will be given instructions about your dressings and stitches when you go home. You will be seen in clinic by Mr Platt and by the nurses for your post operative checks. This will vary depending on your needs but may be up to a year. Post-operative pain is easily controlled. You should be mobile from day one and should be back to full exercise within six weeks. You are recommended to take at least two to four weeks off work immediately after the operation in order to ensure that you recuperate fully.
All breast reductions result in some scarring although the nature of the scars will depend on the technique that has been used. Scars tend to be quite red in the first six weeks, changing to purple over next three months and then fading to white. Most patients will form good quality scars over time, but occasionally and unpredictably some patients will get red lumpy scars that do not improve.
What complications can occur?
Whilst these operations are generally regarded to be highly successful, there are various negatives and complications that patients need to consider. This is a major operation and you must be prepared for the process and recovery period. Most patients are delighted with the physical and cosmetic improvements that breast reduction brings. However, it is impossible to guarantee that a particular cup size will result.
There will be minor asymmetries between your breasts and the scars. Occasionally patients will bleed immediately after the operation and need to go back to the operating room for this to be dealt with. Wound healing problems are quite common, particularly in the anchor scar procedure where the horizontal and vertical scars meet. Most wound problems are minor and can be managed with simple dressings.
However, more major wound problems can arise such as infections, skin loss, wound separation and delayed healing. Sometimes some fat beneath the skin will die. This can result in wound problems or lumpiness that takes time to settle. In some cases, the operation can result in the loss of the nipple. Wound problems, if they occur, can delay your recovery and result in worse scarring.
Some patients will get alteration in the feeling of the breasts, this will often improve after the operation, but it is possible that you will lose feeling in a nipple. After many breast reduction techniques it will still be possible to breast-feed, but this ability might be lost.
Breast Mastopexy
Mastopexy (Breast Uplift or up-lifting of droopy breasts)
Droopiness of the breast is a common legacy of motherhood, nursing and the force of gravity taking their toll, and the effect of pregnancy and a distension of the breasts with milk causes the fibrous bands which support the breasts in their youthful shape to break down and the skin to stretch. With the subsequent shrinking the unsupported breasts settle into the stretched skin and gravity pulls them down. Putting on weight and then losing it can have the same effect. So too does the ageing process, which is why women dislike the appearance of their droopy breasts.
Bilateral Mastopexy. 20 years old. Unhappy with shape of breast. 1 month post op.






Mr Platt uses a variety of techniques to lift and reshape the breast. The shape of the scars is largely determined by the amount of lift required. A small lift can be obtained by the peri areolar technique where there is only a scar around the areolar part of the nipple. Larger lifts will require a vertical scar as well and the largest lifts will require the full anchor or inverted T scar. Internally the breast tissue is shaped and attached to the underlying chest wall to reduce the effects of gravity. If the areola ( the darker skin surrounding the nipple) is too large this can be reduced too. If the breasts are too small as well as droopy, their size can be increased during the operation by placing silicone breast implants underneath the tightened breasts. This is known as mastopexy and augmentation.
What are the consequences?
This is a good operation to improve the appearance of droopy breasts but you would be left with scars, possibly some numbness of your nipples and you may not be able to breast feed again. Usually these scars are fine but they are not invisible and could be noticed by others for example, if you were topless on the beach.
What are the limitations?
Because it is not possible to recreate the natural attachment of the breast to the tissues underneath, a mastopexy alone will not greatly increase the fullness of the breasts above the nipples. Fullness above the nipples can be achieved, however, by increasing the size of the breasts with silicone implants. The extra weight of the silicone implants may accelerate the return of the droopiness of the breasts and in any event there is a tendency for the breast to sink downwards as time goes by. You can lessen the rate at which this happens by supporting your breasts in a bra as much as possible.
What are the risks?
As with any major operation under general anaesthetic, there is a small risk of chest problems particularly if you are a smoker and a small risk of thrombosis of veins in your legs, particularly if you are taking a contraceptive pill. In addition there is a small risk of one or more of the following complications.
Rarely heavy bleeding from the broken blood vessels can occur after the operation, which requires treatment in theatre under another anaesthetic. Occasionally, infection (usually from germs that are lying dormant in the ducts of the breast) can cause part of the wounds to break down which prolongs the healing period and worsens the quality of the final scars.
What you can expect at the time of the operation?
This surgery is carried out under a general anaesthetic and involves an overnight stay. You will be given painkillers for the discomfort you experience in the first few days and will be fitted with an adjustable post-surgery support bra. You should refrain from strenuous physical exercise including swimming, for a month and you will probably require at least two weeks off work. Over the next 6 to 12 months the scars will gradually fade from red to pale. You will be offered regular follow ups by Mr Platt and the nurses.
Please be aware that it is not possible to reshape droopy breasts without significant scars and the lift will not last forever as the effects of gravity and time eventually take their toll.
Breast Mastopexy and Augmentation
Some patients may have a combination of both droopy breasts and lack of volume. This is one of the hardest shapes to improve in cosmetic breast surgery. If the droop is mild and volume is also required, then Mr Platt may advise an internal mastopexy. An internal mastopexy is perform by internal sutures that are placed behind the breast tissue to suspend it against the chest wall.
Where the droop is more severe external scars may be required and can range from a scar just around the nipple (Peri Areolar Mastopexy) with a vertical extension (Lollipop Scar) or anchor type scar. Sometimes it is best to stage the surgery and perform the mastopexy first and the augmentation a few months later. Staging the operation in this fashion can result in less wound breakdown. If you have this type of difficult shape to correct, Mr Platt can go through all of the surgical options with you in clinic and show example photographs.
Gynaecomastia
Gynaecomastia or male breast enlargement is a common condition. For men who feel self-conscious about their appearance, reduction surgery can be helpful. The procedure removes tissue from the breasts, and in extreme cases excess skin.
Gynaecomastia. 25 years old. 2 stage gynaecomastia with large areola treatment. First stage liposuction and excision glandular tissue 2nd stage periareolar reduction. 18 months post 1st stage and 6 monts post 2nd

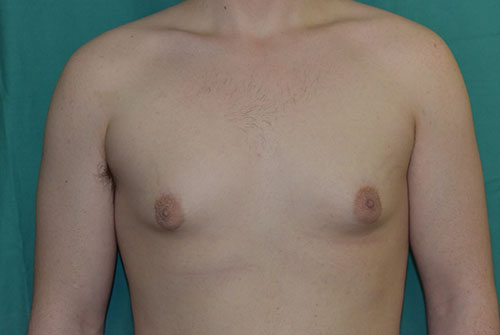




Gynaecomastia. 25 years old. Liposuction and excision of glandular tissue though scar at lower edge of areola. After photos taken one year post surgery.






Gynaecomastia. 40 years old. Liposuction and excision of glandular tissue though scar at lower edge of areola. After photos taken 2 weeks post surgery.






The breast is made up of two main components, glandular tissue (firm and dense) and fatty tissue (soft). The ratio of glandular to fatty tissue in any breast varies from individual to individual and in gynaecomastia there may be an excess of both. For most cases Mr Platt uses a combination of liposuction of the fat and direct excision of the glandular tissue through a scar under the nipple.
Major reductions that involve the removal of a significant amount of tissue and skin may require larger incisions that result in more obvious scars. The surgery is usually carried out under a general anaesthetic with an overnight stay.
Following the surgery the chest is swollen and bruised for a while and it can be difficult to assess the full effect of the operation. To help reduce swelling an elastic pressure garment is continuously worn for several weeks. It is advisable to refrain from exercise for about three weeks and, in general, it takes about six weeks before one can return to completely normal activities. The potential complications of the surgery are relatively rare. They include inadequate removal of breast tissue, an uneven contour to the chest and reduced nipple sensation. If an excision has been performed, rather than liposuction, then a blood clot can form that may need to be drained at a second operation.